
Essential Medications in ACLS Protocols
In Advanced Cardiovascular Life Support, several medications play critical roles in managing cardiac emergencies. These drugs help correct arrhythmias, support circulation, and treat electrolyte imbalances. Proper selection, timing, and dosing are essential for optimizing patient outcomes during resuscitation.
| Drug | Class / Type | Primary Use | Recommended Dosage |
| Adenosine | Antiarrhythmic (Class V) | Termination of stable narrow-complex supraventricular tachycardia (SVT) | 1st dose: 6 mg IV rapid push; 2nd dose: 12 mg IV rapid push if no response within 1-2 minutes |
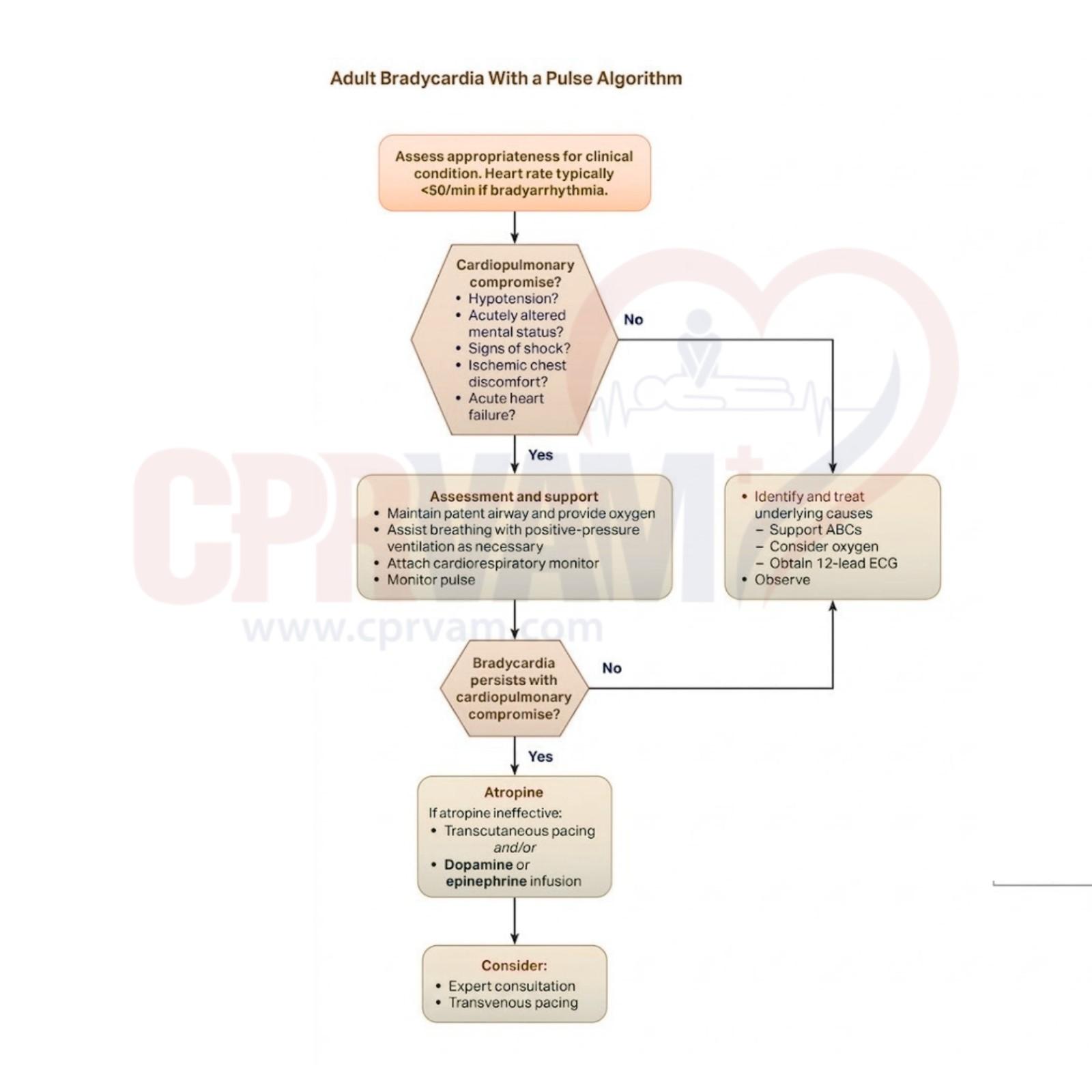
| Epinephrine | Catecholamine (α- and β-adrenergic agonist) | Cardiac arrest (all rhythms), symptomatic bradycardia unresponsive to atropine or pacing | Arrest: 1 mg IV/IO every 3-5 minutes; Bradycardia: infusion 2-10 mcg/min |
| Amiodarone | Antiarrhythmic (Class III) | VF/pulseless VT unresponsive to CPR/defibrillation; stable wide-complex tachycardia | Arrest: 300 mg IV/IO bolus, may repeat 150 mg; Non-arrest: 150 mg over 10 minutes |
| Atropine | Anticholinergic | Symptomatic bradycardia, especially vagally mediated or AV nodal block | 1 mg IV every 3-5 minutes; max total dose 3 mg |
| Lidocaine | Antiarrhythmic (Class IB) | Alternative to amiodarone for refractory VF/pulseless VT | 1-1.5 mg/kg IV bolus; may repeat 0.5-0.75 mg/kg (max cumulative 3 mg/kg) |
| Dopamine | Catecholamine (dopaminergic + α/β agonist) | Symptomatic bradycardia unresponsive to atropine and pacing | Infusion: 5-20 mcg/kg/min, titrated to response |
| Magnesium Sulfate | Electrolyte / Antiarrhythmic | Torsades de Pointes, hypomagnesemia, digoxin toxicity | Torsades: 1-2 g IV over 5-60 minutes; Arrest with hypomagnesemia: 1-2 g IV/IO |