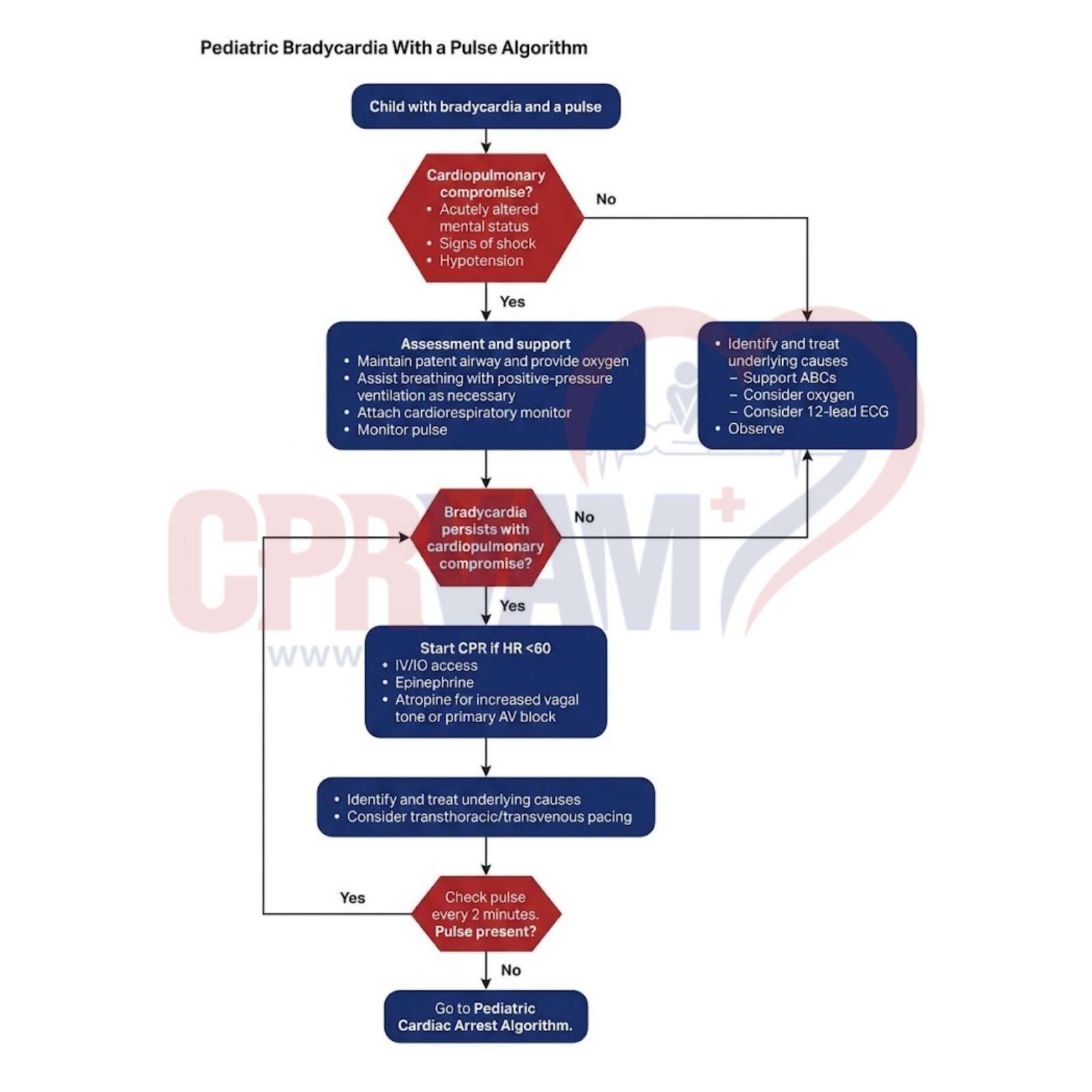
Common Reversible Causes of Pediatric Bradycardia
Pediatric bradycardia often results from reversible conditions that must be quickly identified and corrected. Early recognition helps improve heart rate and overall circulation in the child.
Common causes include:
- Hypothermia
- Hypoxia
- Toxins or medication effects
- Increased intracranial pressure
- Increased vagal tone
- Heart block
- Physiologic or appropriate bradycardia