- 2026
CPR VAM • All Rights Reserved • Developed by Splendour Group


Immediate initiation of resuscitation is essential in cardiac arrest to maintain vital organ perfusion. Begin high-quality CPR without delay while preparing advanced life support equipment.
Essential Actions:
Once monitoring is established, CPR is briefly paused to analyze the cardiac rhythm. This determines whether defibrillation is required or non-shockable arrest management should continue.
Clinical Priorities:
Shockable rhythms such as VF or pulseless VT require immediate defibrillation to restore organized cardiac electrical activity. CPR must resume immediately after shock without delay or pulse check.
Defibrillation Protocol:
After defibrillation or in non-shockable rhythms, continuous high-quality CPR for two minutes is critical to maintain perfusion and prepare for the next rhythm assessment.
CPR Performance Standards:
Drug therapy enhances resuscitation effectiveness. Epinephrine is administered in all cardiac arrest rhythms, while antiarrhythmics are used for refractory shockable rhythms.
Pharmacologic Interventions:
Advanced airway management improves oxygenation and ventilation control during prolonged resuscitation. It enables uninterrupted compressions with reliable airway protection and monitoring.
Airway Management Measures:
CPR effectiveness must be continuously evaluated using end-tidal CO₂ monitoring. Low or decreasing values indicate poor perfusion and require immediate correction of compression quality.
Quality Assurance Measures:
Rhythm is reassessed every two minutes to guide ongoing management decisions, including defibrillation or continuation of CPR with medications and reversible cause evaluation.
Clinical Decision Steps:
Resuscitation follows a continuous structured cycle of CPR, rhythm analysis, defibrillation, medications, and airway management until return of spontaneous circulation or termination of efforts.
Ongoing Resuscitation Strategy:
Advanced airway management in ACLS cardiac arrest involves securing and maintaining a patent airway to ensure adequate ventilation and oxygen delivery during resuscitation. It supports continuous chest compressions, improves respiratory control, and uses verified techniques for tube placement confirmation. Controlled ventilation is provided once the airway is established to optimize perfusion and outcomes.
Key Highlights:
Reversible causes of cardiac arrest, known as the H’s and T’s, represent critical underlying conditions that must be rapidly identified and corrected during resuscitation. Addressing these factors improves the effectiveness of CPR and defibrillation, increases the likelihood of ROSC, and helps prevent ongoing or recurrent cardiac arrest during treatment.
Hypovolemia: Severe loss of blood or fluids leading to reduced circulation
Hypoxia: Inadequate oxygen supply to tissues
Hydrogen ion (Acidosis): Excess acid impairs cardiac function
Hypo-/Hyperkalemia: Abnormal potassium levels causing dangerous arrhythmias
Hypothermia: Critically low body temperature affecting heart activity
Tension Pneumothorax: Air trapped in the chest compressing the lungs and heart
Cardiac Tamponade: Fluid around the heart, limiting cardiac output
Toxins: Drug overdose or poisoning affecting heart function
Thrombosis Pulmonary (PE): A blood clot blocking pulmonary circulation
Thrombosis Coronary (MI): Blockage of a coronary artery causing a heart attack
Return of Spontaneous Circulation (ROSC) occurs when effective cardiac activity resumes after resuscitation, restoring blood flow to vital organs. In the 2025 AHA ACLS algorithm, it indicates successful resuscitation and transition from active CPR to the post–cardiac arrest care management phase.
ROSC is identified by return of a palpable pulse, spontaneous breathing or improved respiratory effort, and rising end-tidal CO₂ levels. Immediate post-cardiac arrest care begins to stabilize the patient, support organ function, treat the underlying cause, and prevent further complications effectively.
Timely and coordinated implementation of the ACLS Cardiac Arrest Algorithm is essential for improving patient survival during cardiac emergencies. High-quality CPR, early defibrillation, accurate rhythm assessment, and appropriate drug therapy work together to increase the chances of achieving return of spontaneous circulation (ROSC).
Identifying and treating reversible causes further increases resuscitation success and prevents recurrence. Proper application of the AHA ACLS algorithm ensures better outcomes in critical emergencies. For structured training and life-saving skill development, visit CPR VAM CPR Training Center.
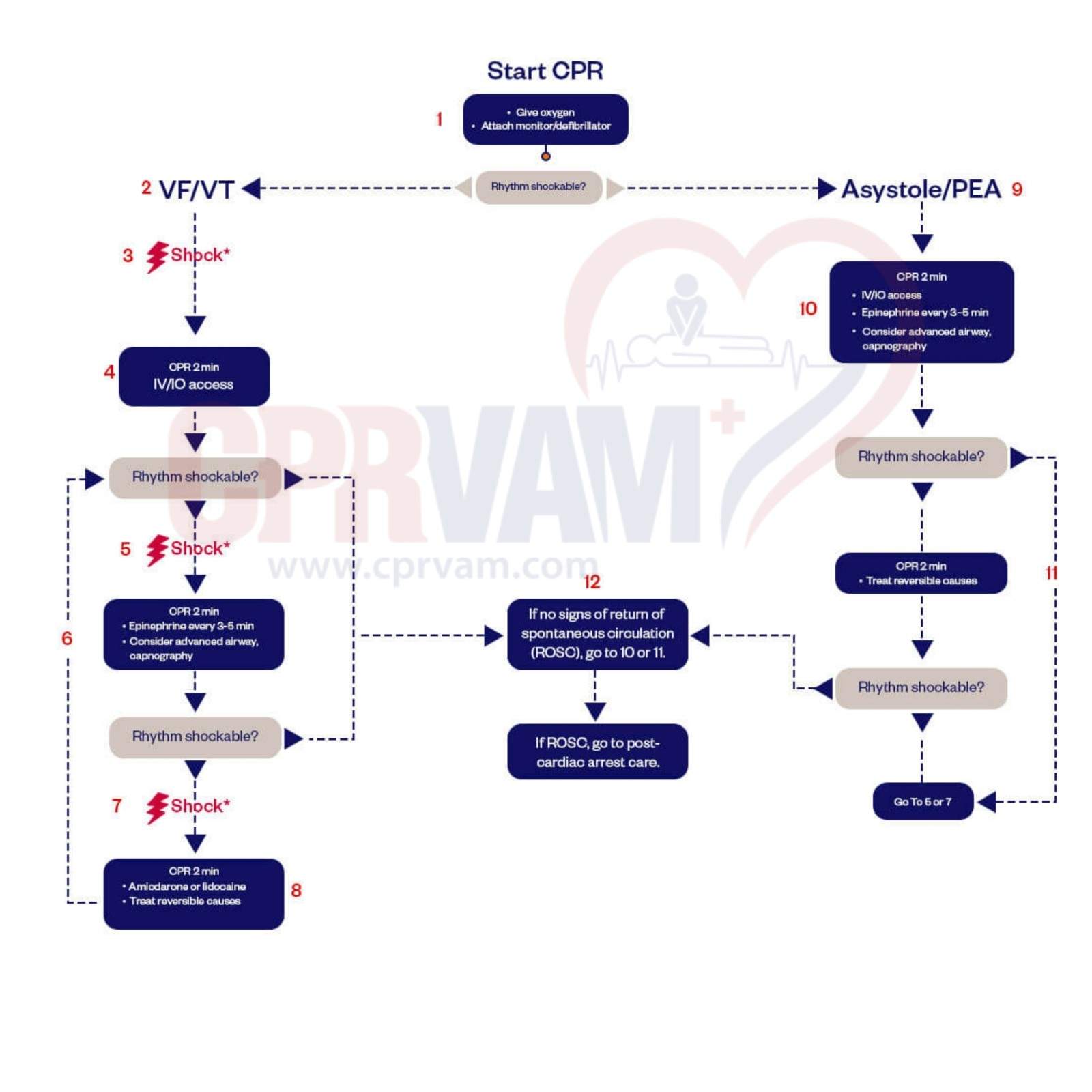
The AHA ACLS Cardiac Arrest Algorithm is a structured, step-by-step guide used by healthcare providers to manage cardiac arrest. It combines high-quality CPR, timely defibrillation, medication administration, advanced airway support, and identification of reversible causes to improve the chances of survival and recovery.
The ACLS cardiac arrest algorithm includes these key steps: start high-quality CPR immediately, check the rhythm to see if it’s shockable, deliver a shock if needed, resume CPR for 2 minutes, give epinephrine every 3–5 minutes, consider advanced airway placement, administer antiarrhythmic drugs if indicated, and identify and treat reversible causes (the H’s and T’s). Continue cycles of CPR and rhythm checks until return of spontaneous circulation (ROSC) or termination of efforts.
Shockable rhythms include ventricular fibrillation and pulseless ventricular tachycardia. Non-shockable rhythms are asystole and pulseless electrical activity. The treatment depends on this classification.
Epinephrine should be administered as soon as IV or IO access is established and then repeated every 3–5 minutes during cardiac arrest to help stimulate the heart and improve blood flow to vital organs.
After ROSC, care focuses on stabilizing the patient by ensuring a clear airway, supporting breathing and blood pressure, monitoring vital signs, and preventing brain injury through treatments like targeted temperature management.