Antiarrhythmic Medications for ACLS Tachycardia Management
Antiarrhythmic drugs restore or control the rhythm in stable tachycardia. They must be carefully dosed and monitored to avoid hypotension, proarrhythmia, or conduction abnormalities during infusion therapy.
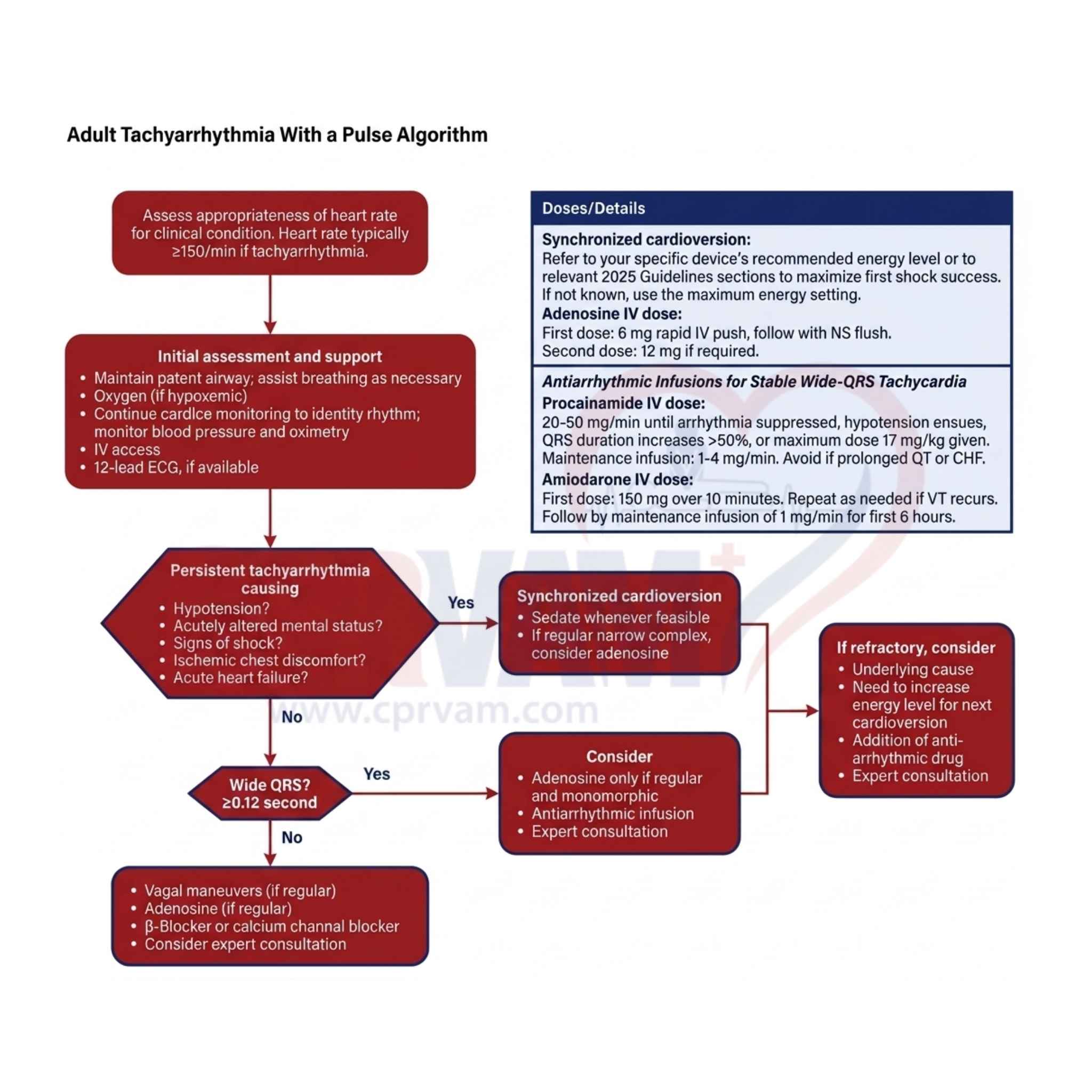
1. Adenosine
Adenosine briefly blocks AV node conduction to terminate regular narrow-complex SVT. It acts rapidly and has a very short duration, given as a fast IV bolus.
Essential Points:
- Used for regular narrow-complex supraventricular tachycardia (SVT)
- Given as 6 mg rapid IV push, then 12 mg if needed
- Temporarily blocks AV node conduction to stop re-entry circuits
- Causes brief flushing, chest discomfort, or transient pause
2. Amiodarone
Amiodarone is a broad-spectrum antiarrhythmic that stabilizes cardiac membranes and slows conduction. It is used in ventricular tachycardia and refractory supraventricular arrhythmias under monitoring.
Core Points:
- Used for ventricular tachycardia and refractory SVT
- Given as 150 mg IV over 10 minutes initially
- Followed by maintenance infusion at 1 mg/min
- May cause hypotension and bradycardia during infusion
3. Procainamide
Procainamide slows sodium channel conduction and prolongs refractoriness. It is mainly used for stable wide-complex tachycardia and requires slow infusion with careful monitoring.
Key Takeaways:
- Used for stable wide-complex tachycardia (suspected VT)
- Infused slowly at 20–50 mg per minute IV
- Maximum total dose is 17 mg/kg
- Avoid in prolonged QT interval and heart failure
4. Sotalol
Sotalol is a beta-blocker with class III antiarrhythmic effects. It prolongs repolarization and is used for stable ventricular and supraventricular tachycardias with ECG monitoring.
Important Points:
- Used for stable ventricular and supraventricular tachycardias
- Has both beta-blocking and potassium channel-blocking effects
- Requires QT interval monitoring to prevent torsades de pointes
- Administered in monitored clinical settings only
5. Beta-blockers (e.g., Metoprolol)
Beta-blockers reduce heart rate by blocking sympathetic stimulation and slowing AV node conduction. They are commonly used for rate control in stable tachycardias.
Main Points:
- Used for rate control in stable tachycardia and atrial fibrillation
- Example includes metoprolol given IV or orally
- Works by blocking beta-adrenergic sympathetic activity
- May cause bradycardia and hypotension if excessive
6. Calcium Channel Blockers (e.g., Diltiazem)
Diltiazem slows AV node conduction and reduces heart rate. It is used in stable supraventricular tachycardia and atrial fibrillation when beta-blockers are not suitable.
Key Points
- Used for stable SVT and atrial fibrillation rate control
- Works by blocking calcium channels in the AV node
- Alternatively, when beta-blockers are contraindicated
- May cause hypotension and bradycardia during use