Key Goals in Managing Pediatric Tachycardia
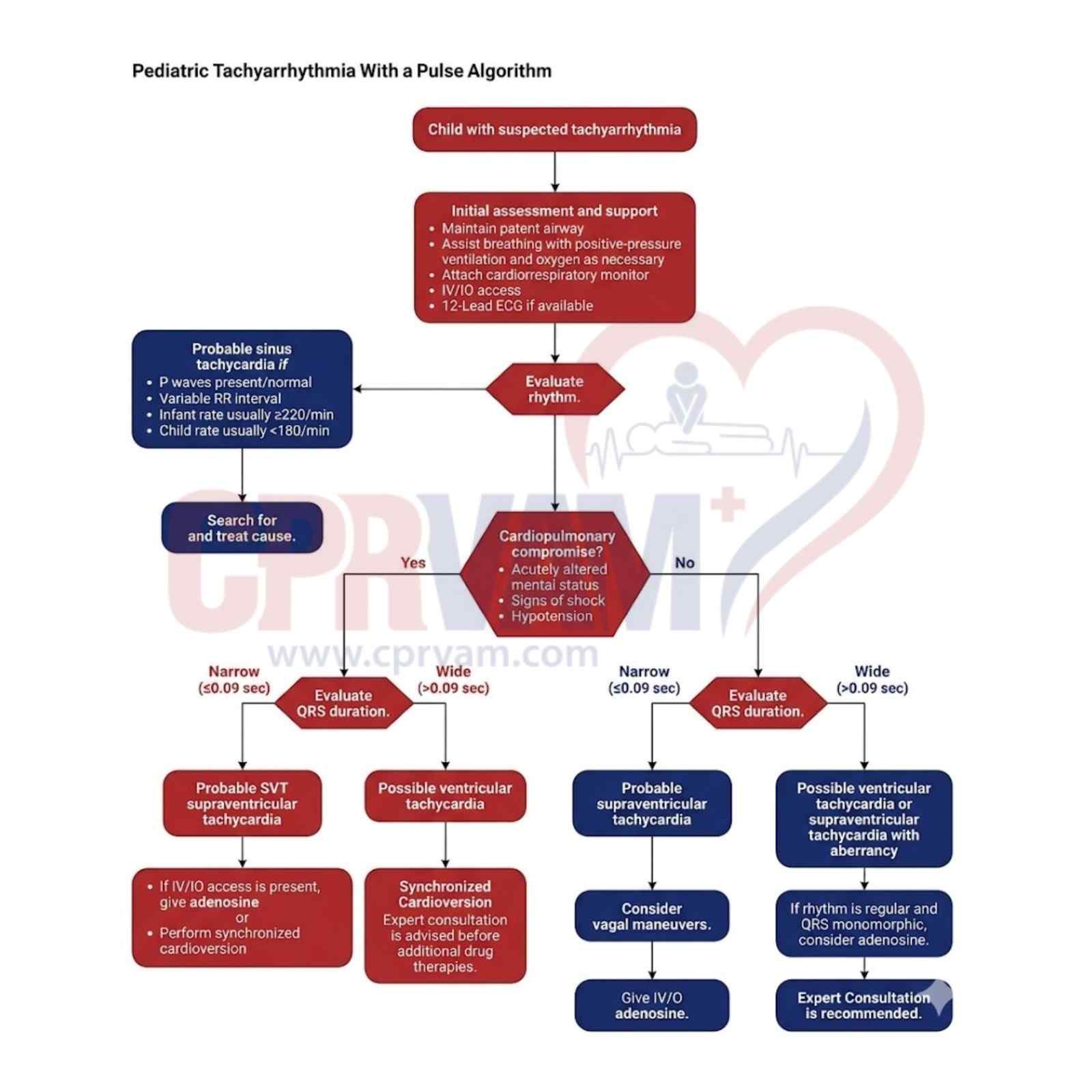
Effective management of pediatric tachycardia, guided by the American Heart Association 2025 approach, focuses on rapid rhythm identification, clinical assessment, and timely intervention. Providers must differentiate between stable and symptomatic cases, recognize underlying causes, and apply appropriate treatments to ensure safe, accurate, and outcome-driven pediatric emergency care.
Key Points:
- Identify the specific tachycardia rhythm (e.g., sinus, SVT, atrial fibrillation)
- Distinguish between narrow and wide complex tachycardia
- Assess if the child has symptomatic tachycardia with a pulse
- Evaluate overall clinical stability and perfusion status
- Treat underlying or reversible causes promptly
- Apply appropriate interventions, including cardioversion if indicated