Clinical Importance of the Cardiac Arrest in Pregnancy Algorithm
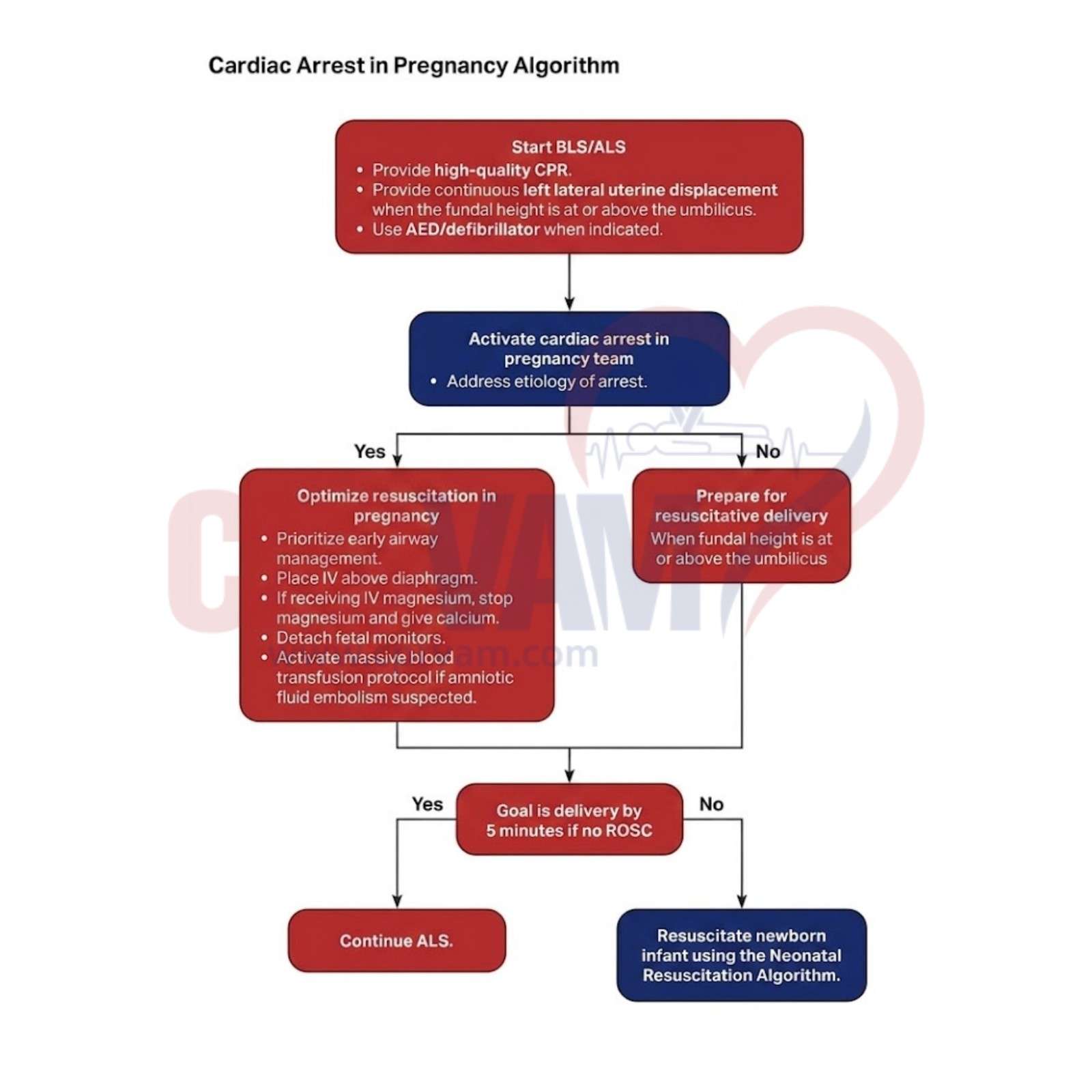
The Cardiac Arrest in Pregnancy Algorithm guides rapid, coordinated resuscitation, ensuring modified CPR, airway management, timely delivery decisions, and multidisciplinary teamwork to improve survival outcomes for both mother and fetus.
Importance of the Cardiac Arrest in Pregnancy Algorithm:
Correction of Hemodynamic Obstruction
The algorithm recommends manual left uterine displacement to relieve aortocaval compression and restore effective blood flow during CPR in pregnancy.Time-Critical Surgical Intervention (5-Minute Rule)
It guides perimortem cesarean delivery if return of spontaneous circulation (ROSC) is not achieved within minutes to improve maternal circulation and fetal survival.Anatomical Modification of Advanced Life Support
It emphasizes IV/IO access above the diaphragm to ensure medications reach central circulation effectively despite uterine compression.Specialized Airway and Oxygenation Strategy
The algorithm calls for early airway management with 100% oxygen due to rapid desaturation and increased aspiration risk in pregnancy.Multi-Specialty Resource Mobilization
It ensures rapid activation of a multidisciplinary team to coordinate simultaneous maternal resuscitation and neonatal preparedness.