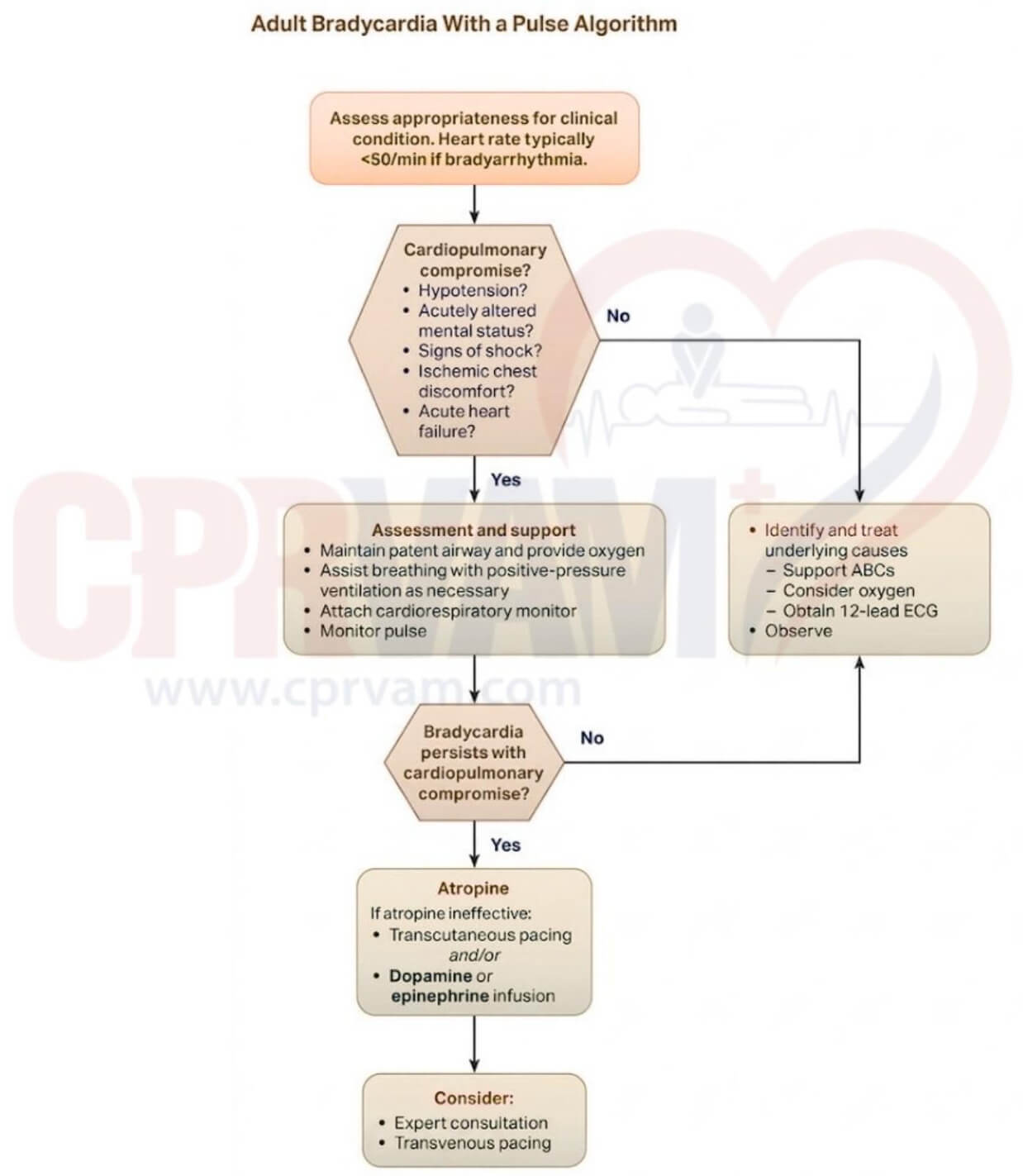
H’s and T’s Reversible Causes in the ACLS Bradycardia Algorithm: Adult Bradycardia With a Pulse
One of the key steps in the ACLS Bradycardia Algorithm is to identify, address, and treat the reversible causes using H’s and T’s mnemonic. Here are the symptoms and treatment for the H’s and T’s reversible causes of bradycardia:
| Reversible Causes | Symptoms | Treatment |
| Hypoxia | Shortness of breath, confusion, cyanosis, and organ dysfunction | Managing the airway and adequate oxygenation |
| Hypovolemia | Low blood pressure, rapid pulse, pale skin | Includes rapid fluid resuscitation with crystalloids or blood products |
| Hydrogen ion (Acidosis) | Respiratory acidosis from CO2 retention; metabolic acidosis from acid accumulation | Correct the underlying cause, ventilation support, and sodium bicarbonate if metabolic |
| Hyperkalemia | High potassium causes peaked T-waves, a widened QRS complex on ECG | Calcium, insulin + glucose, bicarbonate, Kayexalate |
| Hypokalemia | Low potassium causes flattened T-waves and prominent U-waves on ECG | Controlled potassium infusion |
| Hypoglycemia | Sweating, confusion, seizures | IV glucose administration |
| Hypothermia | Impaired metabolism, reduced drug response, arrhythmias | Gradual rewarming, supportive care |
| Toxins (Drug Overdose, Poisoning) | Include altered mental status, ECG changes, or abnormal heart rhythm | Antidotes, supportive care, poison control consultation |
| Tamponade (Cardiac) | Muffled heart sounds, jugular venous distension, hypotension | Treatment by pericardiocentesis to drain fluid |
| Tension Pneumothorax | Respiratory distress, absent breath sounds on the affected side, and distended neck veins | Emergency needle decompression followed by chest tube insertion |
| Thrombosis (Coronary) | Chest pain, dyspnea, hypoxia | Anticoagulation, thrombolysis, supportive care |
| Thrombosis (Pulmonary Embolism) | Severe chest pain, cough, fainting/syncope, leg swelling | Anticoagulants, oxygen, IV fluids, thrombolysis/embolectomy |
| Trauma | Absent pulses, low blood pressure, altered mental status, physical injury that may cause bleeding, organ damage, or airway obstruction | Airway, breathing, circulation stabilization, hemorrhage control |