Importance of the Pediatric Post–Cardiac Arrest Care Algorithm
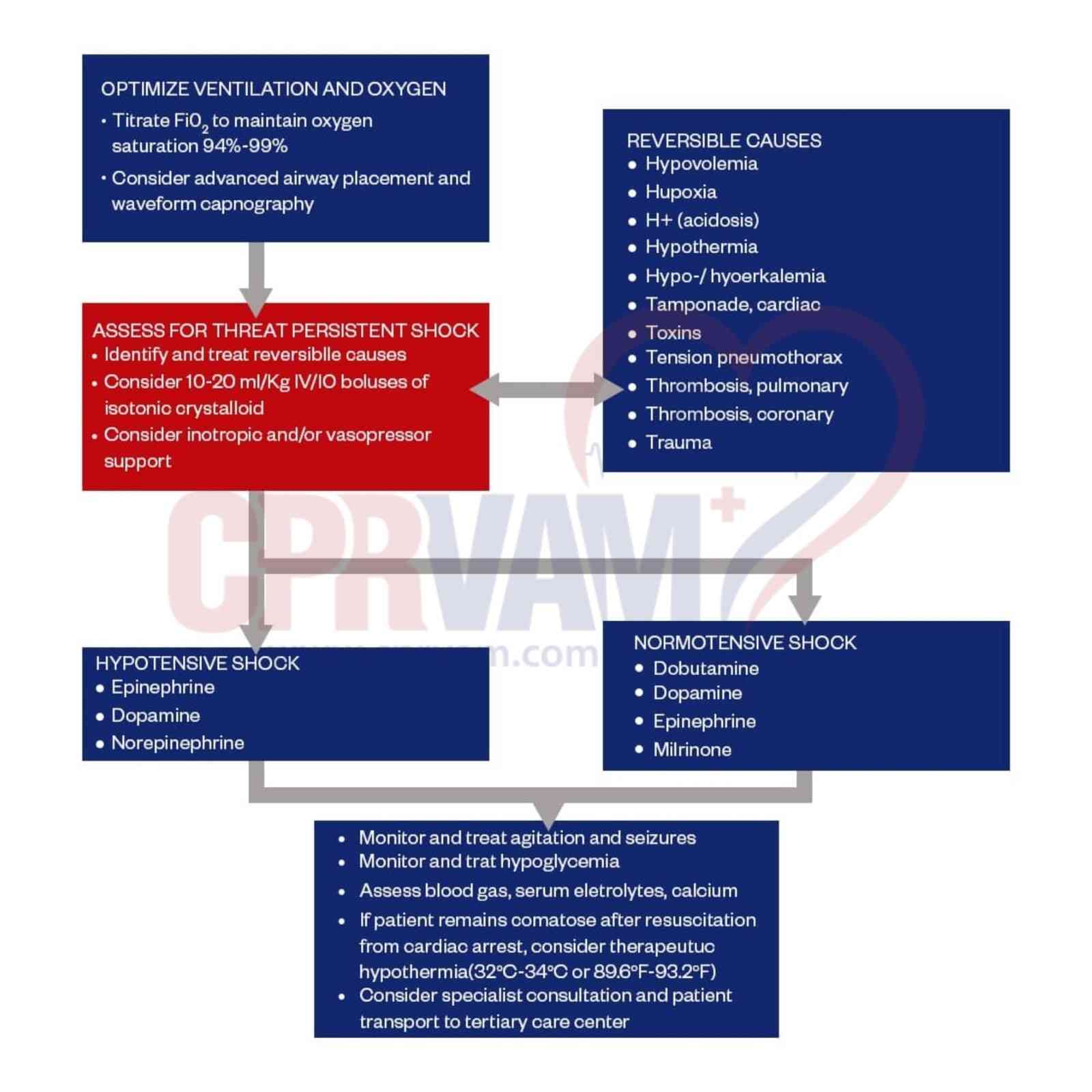
The pediatric post–cardiac arrest care algorithm is a structured, evidence-based framework that guides clinicians in delivering timely and coordinated care after return of spontaneous circulation (ROSC). It focuses on stabilizing vital functions, preventing secondary brain and organ injury, and improving survival and neurological outcomes in children.
Key Importance:
- Ensures systematic and standardized post-ROSC care
- Optimizes oxygenation, ventilation, and tissue perfusion
- Guides hemodynamic stabilization (blood pressure and heart rate control)
- Supports glucose monitoring and metabolic balance
- Enables early identification and treatment of the cause of arrest
- Reduces risk of neurological damage and improves survival outcomes
- Addresses complex pediatric post-cardiac arrest physiology
- Aligns care with evidence-based pediatric resuscitation guidelines
- Enhances clinical preparedness and decision-making in emergencies