Understanding cardiac rhythms is a fundamental skill for healthcare providers, especially those involved in emergency and critical care. Cardiac rhythms represent the electrical patterns that control the heart’s contractions and maintain effective blood circulation throughout the body. Recognizing these rhythms quickly can be the difference between life and death, as each pattern indicates a specific state of cardiac function and guides immediate interventions.
In Advanced Cardiovascular Life Support (ACLS), accurate identification of cardiac rhythms is crucial for effective patient management. Shockable rhythms like Ventricular Fibrillation (VF) and Pulseless Ventricular Tachycardia (VT) require rapid defibrillation, while non-shockable rhythms such as Asystole and Pulseless Electrical Activity (PEA) demand high-quality CPR and prompt treatment of reversible causes. Additionally, bradycardia- and tachycardia-related rhythms guide the use of medications, pacing, or synchronized cardioversion to stabilize patients. Mastering these rhythms improves response time and enhances survival outcomes during cardiac emergencies.
This blog covers all the essential cardiac rhythms you need to know for ACLS, including shockable, non-shockable, bradycardia, and tachycardia-related patterns. By understanding these rhythms, you can make faster, more informed decisions and confidently follow ACLS protocols.
What Are Cardiac Rhythms?
Cardiac rhythms are the patterns of electrical activity that control the heart’s beating and maintain blood flow throughout the body. These rhythms are generated by the heart’s conduction system, including the sinoatrial (SA) node, atrioventricular (AV) node, and the ventricular conduction pathways. On an electrocardiogram (ECG), cardiac rhythms appear as a series of waves and complexes representing atrial and ventricular depolarization and repolarization.
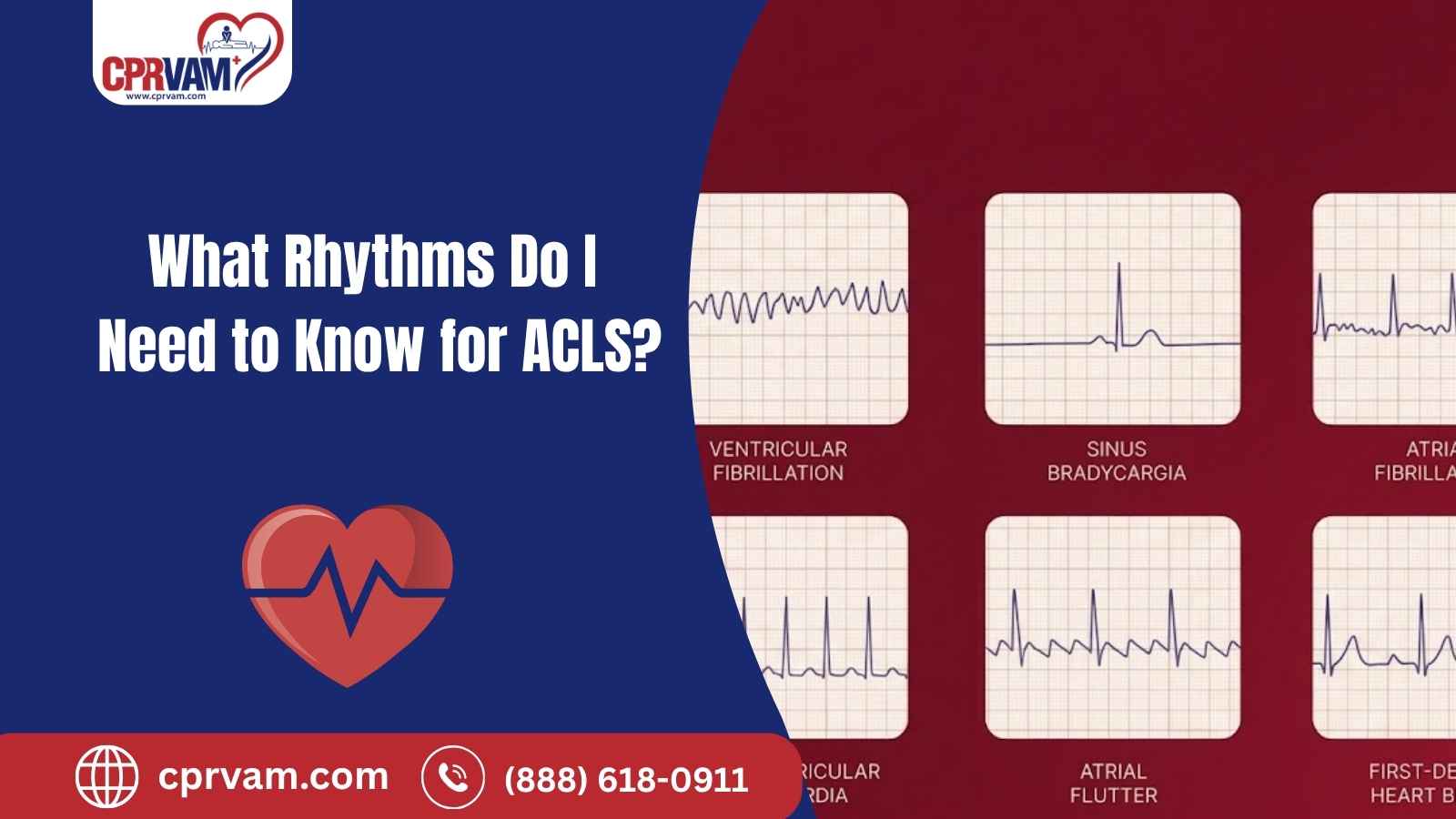
Cardiac rhythms can be categorized into several types, including shockable rhythms like ventricular fibrillation and pulseless ventricular tachycardia, non-shockable rhythms such as asystole and pulseless electrical activity, bradycardia-related rhythms, and tachycardia-related rhythms. Each rhythm has distinct characteristics on the ECG, including heart rate, regularity, QRS width, and P wave appearance. Accurate identification of these rhythms is essential in clinical settings and for ACLS training.
Why Is Cardiac Rhythm Recognition Critical in ACLS?
In ACLS, every second is critical for saving a victim’s life. Accurate cardiac rhythm recognition allows healthcare providers to quickly determine the right intervention during cardiac emergencies. The ECG is more than just lines on a monitor; it’s a roadmap for life-saving decisions.
For example:
Shockable rhythms like ventricular fibrillation (VF) or pulseless ventricular tachycardia (VT) require immediate defibrillation to restore a perfusing rhythm.
Non-shockable rhythms such as asystole or pulseless electrical activity (PEA) require high-quality CPR, medications, and identification of reversible causes.
Bradycardia and tachycardia rhythms guide whether interventions like atropine, pacing, antiarrhythmic medications, or synchronized cardioversion are needed.
A delayed or incorrect interpretation can cost precious time and reduce survival chances. Mastering rhythm recognition ensures healthcare providers can act decisively, follow ACLS algorithms correctly, and improve patient outcomes.
What Are the Core ACLS Rhythms to Know?
In ACLS, recognizing the core cardiac rhythms is essential because each one dictates a specific treatment strategy. These rhythms are categorized into shockable, non-shockable, bradycardia-related, and tachycardia-related rhythms. Understanding them thoroughly ensures you can respond quickly and appropriately during cardiac emergencies.
1. Shockable Rhythms
Shockable rhythms are life-threatening arrhythmias that respond to defibrillation. Recognizing these rhythms quickly is critical, as immediate action can save a patient’s life.
In ACLS, there are two primary shockable rhythms:
A. Pulseless Ventricular Tachycardia (VT)
Pulseless Ventricular Tachycardia (VT) is a rapid, wide-complex rhythm without a detectable pulse, meaning the heart isn’t pumping effectively. It is shockable, so immediate defibrillation and CPR are essential. Medications like epinephrine and amiodarone may be given to help restore a stable rhythm. Prompt recognition and treatment are critical to prevent cardiac arrest.
B. Ventricular Fibrillation (VF)
Ventricular Fibrillation (VF) is a life-threatening rhythm where the ventricles quiver instead of contracting, stopping effective blood flow. On an ECG, it appears as a chaotic, irregular waveform with no clear QRS complexes. VF is shockable, so immediate defibrillation and high-quality CPR are critical. Medications like epinephrine and amiodarone may be used to stabilize the rhythm, and airway support may be needed. Quick recognition and action greatly improve survival chances.
2. Non-Shockable Rhythms
Non-shockable rhythms are cardiac arrhythmias that do not respond to defibrillation, so treatment focuses on high-quality CPR, medications, and identifying reversible causes. Prompt recognition is crucial to guide effective interventions and improve patient outcomes.
In ACLS, the two main non-shockable rhythms are asystole and pulseless electrical activity (PEA).
A. Pulseless Electrical Activity (PEA)
Pulseless Electrical Activity (PEA) is a condition where the heart shows organized electrical activity on the ECG, but there is no palpable pulse or effective circulation. Since the heart isn’t pumping blood, defibrillation is not indicated.
Management focuses on immediate, high-quality CPR, administration of epinephrine, and identifying reversible causes, often remembered as the Hs and Ts (hypovolemia, hypoxia, hydrogen ion [acidosis], hypo-/hyperkalemia, tension pneumothorax, tamponade, toxins, and thrombosis). Rapid recognition and intervention are essential to improve the chances of patient survival.
B. Asystole
Asystole is a complete absence of electrical activity in the heart, appearing as a flatline on the ECG. Since there is no organized rhythm, defibrillation is not effective. Treatment focuses on immediate high-quality CPR, administration of epinephrine, and identifying reversible causes such as hypoxia, severe acidosis, or electrolyte imbalances. Rapid action is essential, as asystole is associated with a very low survival rate without prompt intervention.
3. Bradycardia-Related Rhythms
Bradycardia-related rhythms occur when the heart beats slower than normal, usually under 60 beats per minute. In ACLS, recognizing these rhythms is crucial because some are benign, while others can reduce cardiac output, cause hypotension, or even lead to cardiac arrest if not treated promptly.
Below are the key bradycardia-related rhythms:
A. Sinus Bradycardia
Sinus bradycardia is a slow but regular heart rhythm, typically under 60 beats per minute. It often occurs in healthy individuals, athletes, or during sleep and may not require treatment if the patient is stable. However, if symptoms like dizziness, low blood pressure, or chest discomfort appear, medical intervention may be necessary. Treatment options can include atropine, dopamine, or epinephrine, and in severe cases, temporary pacing may be required to maintain adequate circulation.
B. First-Degree AV Block
First-degree AV block is a rhythm in which all electrical impulses from the atria reach the ventricles, but with a consistent delay. This appears on the ECG as a prolonged PR interval. Usually, it is benign and does not require treatment if the patient is stable. Intervention is only needed if the patient develops symptoms such as dizziness, fatigue, or low blood pressure, in which case medications or monitoring may be considered.
C. Second-Degree AV Block (Type I - Wenckebach)
Also known as Mobitz Type I, this rhythm is characterized by progressively lengthening PR intervals on the ECG until a beat is eventually dropped. It is often benign, especially in asymptomatic patients. Treatment is usually not required unless the patient shows symptoms like dizziness, fatigue, or hypotension, in which case atropine or temporary pacing may be considered.
D. Second-Degree AV Block (Type II)
Also called Mobitz Type II, this rhythm is more serious than Type I. Here, some atrial impulses fail to conduct to the ventricles without warning, leading to sudden dropped beats. It can progress to complete heart block and often requires immediate intervention, typically temporary pacing, even if the patient is only mildly symptomatic. Prompt recognition and treatment are essential to prevent hemodynamic instability.
E. Third-Degree (Complete) Heart Block
In a third-degree heart block, there is a complete dissociation between atrial and ventricular activity. The atria and ventricles beat independently, and the ventricles rely on a slow escape rhythm that often cannot maintain adequate circulation. This rhythm is life-threatening and requires immediate intervention, usually temporary pacing, with consideration for a permanent pacemaker. Rapid recognition and treatment are crucial to prevent severe hypotension, shock, or cardiac arrest.
4. Tachycardia-Related Rhythms
Tachycardia-related rhythms involve a faster-than-normal heart rate, typically above 100 beats per minute. Accurate identification is essential in ACLS, as these rhythms can range from relatively harmless to life-threatening, and treatment decisions depend on both the type of rhythm and patient stability.
Here are the main tachycardia-related rhythms:
A. Atrial Fibrillation (Afib)
Atrial fibrillation is an irregular, often rapid heart rhythm characterized by absent or chaotic P waves on the ECG. This rhythm can reduce cardiac efficiency and lead to poor perfusion. In ACLS, treatment depends on the patient’s condition: stable patients may receive rate control with medications such as beta-blockers or amiodarone, while unstable patients require immediate synchronized cardioversion to restore an effective rhythm.
B. Atrial Flutter
Atrial flutter is a rapid, organized atrial rhythm that appears as a “sawtooth” pattern on the ECG. Like atrial fibrillation, it can reduce cardiac output and cause symptoms such as dizziness, palpitations, or hypotension. In ACLS, treatment depends on stability: stable patients may receive rate control or antiarrhythmic medications, while unstable patients require immediate synchronized cardioversion to restore normal rhythm.
C. Supraventricular Tachycardia (SVT)
Supraventricular tachycardia (SVT) is a rapid, narrow-complex rhythm that originates above the ventricles. Patients may experience palpitations, dizziness, chest discomfort, or shortness of breath. In ACLS, treatment depends on the patient’s stability: stable patients may be managed with vagal maneuvers or adenosine, while unstable patients require immediate synchronized cardioversion to restore a normal heart rhythm.
D. Monomorphic Ventricular Tachycardia (with a pulse)
Monomorphic ventricular tachycardia (VT) with a pulse is a wide-complex, rapid rhythm where each QRS complex looks similar. The patient still has a detectable pulse, but may experience low blood pressure, chest pain, or altered mental status. In ACLS, treatment depends on stability: stable patients may receive antiarrhythmic medications like amiodarone, while unstable patients require immediate synchronized cardioversion to restore a perfusing rhythm.
E. Polymorphic VT / Torsades de Pointes
Polymorphic ventricular tachycardia, often called Torsades de Pointes, is a rapid, twisting, wide-complex rhythm typically associated with prolonged QT intervals or electrolyte imbalances. If the patient has no pulse, it is treated like ventricular fibrillation with immediate defibrillation and CPR. If a pulse is present, magnesium sulfate is the first-line treatment, alongside correcting underlying causes such as low potassium or magnesium levels. Prompt recognition and intervention are critical to prevent sudden cardiac arrest.
What Are the Rhythms That Can Confuse You on the Exam?
Some ECG rhythms appear alarming at first glance but do not follow standard ACLS arrest or tachycardia algorithms. These rhythms are frequently used in exams to test whether you can recognize when no aggressive ACLS intervention is required. Misinterpreting them can lead to incorrect answers or unnecessary treatment.
1. Accelerated Junctional Rhythm
Accelerated junctional rhythm originates from the AV junction and typically presents with a regular rate of 60–100 beats per minute, narrow QRS complexes, and absent or inverted P waves. It often appears on ACLS exams because it can be mistaken for sinus rhythm or supraventricular tachycardia. This rhythm is usually benign, does not follow an ACLS arrest algorithm, and requires no treatment unless the patient is symptomatic.
2. Idioventricular Rhythm
Idioventricular rhythm is a slow ventricular escape rhythm, usually with a heart rate of 20–40 beats per minute, wide QRS complexes, and absent P waves. It often occurs after myocardial infarction or during reperfusion and can be mistaken for ventricular tachycardia on exams. Typically, it is benign and does not require aggressive ACLS interventions unless the patient is unstable, in which case pacing or supportive care may be needed.
3. Artifact
An artifact is a false or misleading ECG pattern caused by external factors such as patient movement, loose leads, or electrical interference. It can mimic serious rhythms like ventricular fibrillation or tachyarrhythmias, but the patient usually shows normal signs and a palpable pulse. In ACLS, recognizing artifacts is crucial to avoid unnecessary interventions, so always confirm the patient’s condition and check lead placement before initiating treatment.
What Are The Tips for Enhancing ACLS Rhythm Interpretation Skills?
Developing strong ACLS rhythm interpretation skills takes consistent practice, reliable learning resources, and up-to-date clinical knowledge. Because ACLS guidelines evolve and rhythm recognition requires speed and accuracy, ongoing skill reinforcement is essential for both exam success and real-world performance.
Below are the tips that you can use to enhance your ACLS Rhythm Interpretation Skills:
1. Practice ECG Rhythm Interpretation Regularly
Regular, repeated practice is the foundation of mastering ACLS rhythms. Reviewing ECG strips daily, even for short periods, helps reinforce pattern recognition and improve response time during emergencies.
Effective practice strategies include:
- Interpreting unlabeled rhythm strips
- Timing yourself to simulate real ACLS scenarios
- Verbalizing the rhythm name and the next appropriate ACLS action
Frequent exposure builds confidence and reduces hesitation during high-pressure situations.
2. Use High-Quality ACLS Learning Resources
Leveraging multiple educational resources strengthens understanding and retention of ACLS rhythms. Each resource offers a different perspective that reinforces learning.
Recommended resources include:
- ACLS textbooks and provider manuals
- Online ACLS courses and ECG interpretation modules
- Simulation tools and rhythm recognition apps
- Practice exams and case-based scenarios
Using a variety of tools helps bridge the gap between theory and clinical application.
3. Participate in Simulation and Scenario-Based Training
Simulation-based training is one of the most effective ways to enhance rhythm interpretation skills. Practicing in realistic scenarios improves decision-making, teamwork, and rapid rhythm identification.
Simulation allows learners to:
- Practice recognizing rhythms under stress
- Apply ACLS algorithms in real time
- Improve confidence in leadership and communication
These skills directly translate to better performance during actual cardiac emergencies.
4. Stay Current With ACLS Guidelines and Updates
ACLS protocols and treatment recommendations are periodically updated. Staying informed ensures your rhythm interpretation aligns with current best practices.
To stay updated:
- Review the latest American Heart Association (AHA) ACLS guidelines
- Attend recertification courses and continuing education sessions
- Follow reputable professional organizations and training providers
Current knowledge ensures you apply the correct interventions for each rhythm.
5. Connect Rhythm Recognition to Clinical Decision-Making
ACLS rhythm interpretation is not just about identifying waveforms; it’s about knowing what to do next. Practice linking each rhythm to its corresponding ACLS algorithm and treatment pathway.
Ask yourself:
- Is the patient stable or unstable?
- Is this rhythm shockable or non-shockable?
- What is the immediate next intervention?
This approach strengthens clinical judgment and improves patient outcomes.
Take Action and Master Life-Saving Rhythms
In conclusion, mastering ACLS cardiac rhythms is a critical skill for healthcare providers, as accurate recognition directly impacts patient outcomes during cardiac emergencies. By understanding shockable and non-shockable rhythms, as well as bradycardia- and tachycardia-related patterns, clinicians can make rapid, informed decisions that follow ACLS algorithms. Continuous practice, use of high-quality learning resources, participation in simulations, and staying updated with current guidelines all enhance rhythm interpretation skills
To take your skills to the next level, join an ACLS certification or recertification class with CPR VAM. CPR VAM offers American Heart Association–approved CPR, ACLS, BLS, and PALS courses designed to equip healthcare providers with practical, life-saving expertise. With experienced instructors, hands-on simulations, and up-to-date training aligned with AHA guidelines, CPR VAM ensures you gain the confidence and authority to act decisively in real emergencies.
Secure your place today and strengthen your ability to save lives when it matters most.
FAQs
1. How Quickly Should I Identify a Cardiac Rhythm During ACLS?
Rhythm recognition should occur within 10 seconds of assessing the patient to ensure timely interventions like defibrillation, CPR, or pacing.
2. Do All Tachycardia Rhythms Require Immediate Treatment?
No. Some, like sinus tachycardia or accelerated junctional rhythm, may be benign. Treatment depends on patient stability, symptoms, and underlying cause.
3. How Do Electrolyte Imbalances Affect ACLS Rhythms?
Imbalances such as hypokalemia, hyperkalemia, or low magnesium can trigger arrhythmias like Torsades de Pointes or VT. Correcting these underlying issues is critical alongside ACLS interventions.
4. Can ACLS Rhythm Recognition Rely Solely on Automated Monitors?
No. While automated ECG analysis can help, clinical judgment and manual verification are essential to avoid misdiagnosis and inappropriate treatment.
5. How Important is Team Communication During ACLS Rhythm Management?
Extremely important. Clear communication and role assignment ensure coordinated actions, compressions, airway management, and defibrillation, reducing errors and improving patient survival.